Source: After J Olesen et al: The Headaches. Philadelphia, Lippincott Williams & Wilkins, 2005
Anatomy
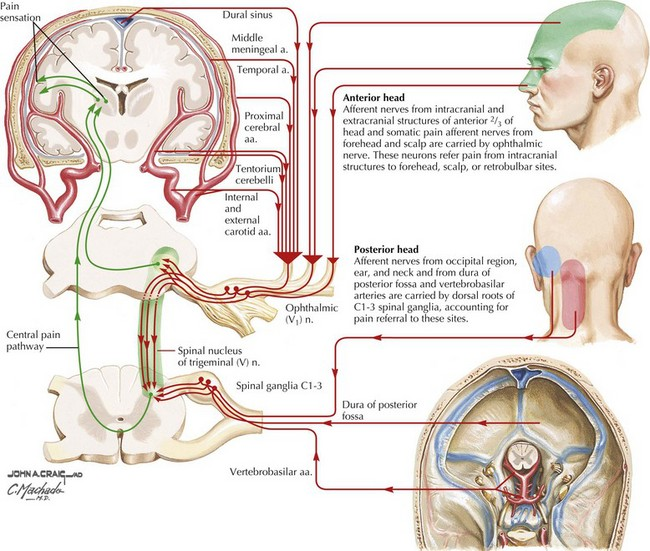
The key structures involved in primary headaches are the following:
The large intracranial vessels and dura mater, and the peripheral terminals of the trigeminal nerve that innervate these structures
The caudal portion of the trigeminal nucleus, which extends into the dorsal horns of the upper cervical spinal cord and receives input from the first and second cervical nerve roots (the trigeminocervical complex)
Rostral pain-processing regions, such as the ventroposteromedial thalamus and the cortex
The pain-modulatory systems in the brain that modulate input from the trigeminal nociceptors at all levels of the pain-processing pathways and influence vegetative functions, such as the hypothalamus and brainstem
From Netter
From Netter
Primary Headache evaluation
Classification of Daily or Near-Daily Headache
Primary
>4 H DAILY
<4 H DAILY
SECONDARY
Chronic migraine (a)
Chronic cluster headache (b
)
Posttraumatic
Head injury
Iatrogenic
Postinfectious
Hemicrania continua
Chronic paroxysmal hemicrania
Inflammatory, such as
Giant cell arteritis
Sarcoidosis
Behçet’s syndrome
Hemicrania continua (a)
SUNCT/SUNA
Chronic CNS infection
New daily persistent headache (a)
Hypnic headache
Medication-overuse headache (a)
From Harrisons IM
a May be complicated by medication overuse. b Some patients may have headaches>4 h/d.
Treatment of Primary Headaches
r/o emergency
r/o secondary headaches
Types
Chronic migraine
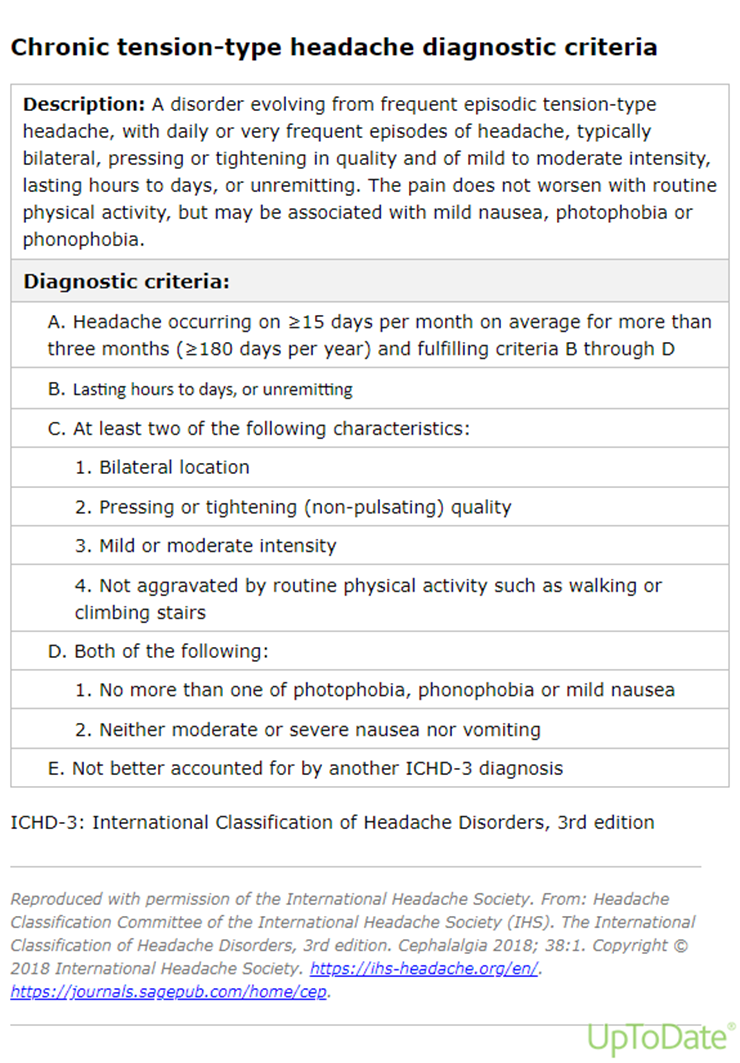
Chronic tension-type headache
Medication overuse headache
Hemicrania continua
New daily persistent headache (NDPH)
Chronic Migraine
Chronic Tension-type Headaches
Management of Medication Overuse: Outpatients
One approach is to reduce the medication dose by 10% every 1–2 weeks. Immediate cessation of analgesic use is possible for some patients, provided there is no contraindication. Both approaches are facilitated by the use of a medication diary maintained during the month or two before cessation; this helps to identify the scope of the problem. A small dose of a nonsteroidal anti-inflammatory drug (NSAID) such as naproxen, 500 mg bid, if tolerated, will help relieve residual pain as analgesic use is reduced. NSAID overuse is not usually a problem for patients with daily headaches when an NSAID with a longer half-life is taken once or twice daily; however, overuse problems may develop with shorter-acting NSAIDS. Once the patient has substantially reduced analgesic use, a preventive medication should be introduced.
Another widely used approach is to commence the preventive at the same time the analgesic reduction is started.
It must be emphasized that preventives may not work in the presence of analgesic overuse, particularly with opioids. The most common cause of unresponsiveness to treatment is the use of a preventive when analgesics continue to be used regularly. For some patients, discontinuing analgesics is very difficult; often the best approach is to inform the patient that some degree of headache is inevitable during this initial period.
Management of Medication Overuse: Inpatients
Antiemetics and fluids;
clonidine is used for opioid withdrawal symptoms.
For acute intolerable pain during waking hours, aspirin, 1 g IV (not approved in the United States), is useful.
IM chlorpromazine can be helpful at night; patients must be adequately hydrated.
Three to five days into the admission, as the effect of the withdrawn substance wears off, a course of IV dihydroergotamine (DHE) can be used. DHE, administered every 8 h for 5 consecutive days, a treatment that is not stopped short if the headache settles, can induce a significant remission that allows a preventive treatment to be established. Serotonin 5-HT3 receptor antagonists, such as ondansetron or granisetron, or the neurokinin receptor antagonist, aprepitant, may be required with DHE to prevent significant nausea, and domperidone (not approved in the United States) orally or by suppository can be very helpful. Avoiding sedating or otherwise side effect–prone antiemetics is helpful.